Narratives on Collaboration: Optimizing Management of Immune-Related Adverse Events
An increasing number of cancer patients are receiving therapy that targets immune checkpoints. These agents represent a remarkable advance in cancer care but are associated with characteristic immune-related adverse events (irAEs) that are driven by the same mechanisms responsible for their therapeutic effects. While most of these toxicities are mild to moderate, some can be serious and potentially life-threatening. As such, it is critical for oncology clinicians to anticipate, monitor for, and manage irAEs appropriately. This is a daunting task that requires mastering an evolving body of knowledge for a newer class of drugs about which few clinicians have received formal training. Narratives on Collaboration: Optimizing Management of Immune-Related Adverse Events—an interactive digital monograph certified for continuing education credit—is thus being offered to improve the ability of oncology advanced practice providers to provide high-quality care for patients treated with immune checkpoint inhibitors.
Release date: July 12, 2019
Expiration date: July 12, 2020
Estimated time to complete activity: 1.0 hour
Fee: None
This activity is designed to help clinicians achieve specific learning objectives, which reflect the desired results of the education. Participants are encouraged to integrate what they learn from this activity into practice to improve patient care and outcomes.
Jointly provided by
In collaboration with
Faculty
Marianne J. Davies, DNP, CNS, ACNP, AOCNP®, Yale University School of Nursing, Yale Comprehensive Cancer Center, Smilow Cancer Hospital at Yale New Haven Hospital, New Haven, Connecticut
Kristen Crowley, MSN, APRN, Yale Comprehensive Cancer Center, Smilow Cancer Hospital at Yale New Haven Hospital, New Haven, Connecticut
Guest Presenter
Nancy Taylor, ADN, Patient
Intended Participants
This activity is designed for community-based oncology clinicians, including nurse practitioners, physician assistants, clinical nurse specialists, advanced practice nurses, and clinical pharmacists, who provide care for patients treated with immune checkpoint inhibitors. Clinicians interested in mitigating irAEs may also wish to participate.
Learning Objectives
After completing this educational activity, participants should be better able to:
Identify key characteristics associated with irAEs, including body systems affected and timing of emergence
Plan strategies to monitor for irAEs
Apply evidence-based best practices to manage irAEs
Devise strategies for providing patient-centered education and counseling regarding irAE self-management
Select approaches to engage patients in monitoring for and managing irAEs
Continuing Education
Certification
This activity is certified for credit by: Annenberg Center for Health Sciences at Eisenhower
39000 Bob Hope Drive, Dinah Shore Bldg.
Rancho Mirage, CA 92270
Voice: 760-773-4500
Fax: 760-773-4513
E-mail: contactce@annenberg.net
Participants who successfully complete this activity—which includes submitting a completed pre-test, submitting and scoring at least 70% on the post-test, and submitting a completed evaluation form—will be able to download a statement of credit.
Physicians. This activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education through the joint providership of the Annenberg Center for Health Sciences at Eisenhower and Harborside Medical Education. The Annenberg Center is accredited by the ACCME to provide continuing medical education for physicians.
The Annenberg Center for Health Sciences at Eisenhower designates this enduring activity for a maximum of 1.0 AMA PRA Category 1 Credit™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Nurses. Annenberg Center for Health Sciences is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center's Commission on Accreditation.
A maximum of 1.0 contact hour may be earned for successful completion of this activity.
Provider is approved by the California Board of Registered Nursing, Provider No. 13664, for 1.0 contact hour.
Pharmacists.
The Annenberg Center for Health Sciences at Eisenhower is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education. This program has been assigned ACPE Universal Program #0797-9999-19-061-H04-P. This program is designated for up to 1.0 contact hour (0.10 CEU) of continuing pharmacy education credit. This is a knowledge-based activity.
Disclosures
Commercial Support
This activity is supported by an educational grant from Bristol-Myers Squibb Company.
Relationships of Faculty and Planners
All individuals in a position to control the content of this activity (e.g., planners, faculty, reviewers) must disclose all financial relationships with commercial interests that may have a bearing on its subject matter. Annenberg Center for Health Sciences at Eisenhower has identified and resolved all conflicts of interest in accordance with its policies and procedures. Participants should assess the impact (if any) of the disclosed information on the educational value of the activity.
Faculty and Guest Presenter
Dr. Davies has served on speakers bureaus for AstraZeneca, Bristol-Myers Squibb Company, Genentech, and Merck.
Ms. Crowley has served on speakers bureaus for Celgene, Exelixis, and Janssen Oncology.
Ms. Taylor has nothing to disclose.
Planners and Reviewers
The staff of and consultants for the Annenberg Center for Health Sciences at Eisenhower and HSME have nothing to disclose.
Product Disclosure
This activity may include discussion of agents that have not yet been approved by the U.S. Food and Drug Administration and investigational uses of approved products. Please consult prescribing information and practice guidelines for detail regarding safe and effective use of therapeutic agents.
Disclaimer
The opinions expressed in this activity are those of the faculty and do not represent an endorsement by Annenberg Center for Health Sciences at Eisenhower of any therapeutic agent or approach to diagnosis or patient management.
Narratives on Collaboration
Optimizing Management of Immune-Related Adverse Events
1.0 Credit
Release Date: July 12, 2019|Expiration Date: July 12, 2020
Yale University School of Nursing, Yale Comprehensive Cancer Center, Smilow Cancer Hospital at Yale New Haven Hospital
Kristen Crowley
MSN, APRN
Yale Comprehensive Cancer Center, Smilow Cancer Hospital at Yale New Haven Hospital
Guest Presenter
Nancy Taylor, ADN
Patient
In this special CE/CME-certified JADPRO monograph, authors Marianne Davies and Kristen Crowley discuss best practices in the management of adverse events often experienced by patients receiving immune checkpoint inhibitor (ICI) therapy. As you read the monograph, you'll learn even more through videos in which the authors share their clinical insights into the role of the oncology advanced practice provider (APP) in supporting patients through their ICI treatment journey. In a special appearance, Nancy Taylor, a patient who currently receives treatment at the authors' institution, gives her perspective on how APPs can best support their patients receiving ICIs. In addition, you'll find two downloadable and reproducible tools for your patients, as well as a list of resources to help both you and your patients learn more.
Davies, M., & Crowley, K. (2019). Optimizing management of immune-related adverse events. Journal of the Advanced Practitioner in Oncology. https://doi.org/10.6004/jadpro.2019.10.5.9.
The introduction of immune checkpoint inhibitors (ICIs) for the treatment of cancer represents a significant advancement in patient care, and the role of these agents continues to expand. Since the US Food and Drug Administration (FDA) granted approval for ipilimumab in 2011 for the treatment of metastatic melanoma, 6 additional checkpoint inhibitors have been approved to treat more than 10 types of cancer. As checkpoint inhibitors address a process central to the proliferation of many types of cancer, the number of indications continues to grow. In addition to the treatment of both hematologic malignancies and solid tumors as single agents, ICIs have been evaluated in combination with other ICIs, cytotoxic agents, other small molecules, and radiation therapy. Emerging evidence regarding ICI therapy continues to shape and reshape the treatment landscape.
However, while the advent of the ICI era has opened the door for new paradigms in the way cancer is treated, ICIs are not without toxicities (from mild to severe, and from immediate to late onset) related to general immunologic enhancement. When adverse events (AEs) arise, clinicians should maintain a high level of suspicion that they may be treatment related (National Comprehensive Cancer Network [NCCN], 2019). Prompt assessment and treatment of these immune-related adverse events (irAEs) are required to ensure that patients receive optimal benefit from these agents.
The purpose of this monograph is to provide evidence-based guidance and experience-based clinical insights to help advanced practice providers (APPs) work in a collaborative practice model to improve quality of care and outcomes for patients treated with ICIs through careful selection of therapy, astute monitoring of treatment response, and efficient identification and management of AEs. This information is particularly valuable for APPs in community practice, as they often see patients with a wide range of malignancies, and may not have the benefit of as many opportunities for on-site education as their counterparts who practice in an academic and/or comprehensive cancer center setting. Additionally, this monograph aims to help APPs empower their patients regarding self-care, use clinical practice resources and tools more widely, and anticipate the clinical significance of emerging data related to ICI therapy.
In addition to the monograph, this activity includes several short videos featuring the authors, Marianne J. Davies, DNP, CNP, ACNP, AOCNP®, and Kristen Crowley, MSN, APRN, discussing their clinical experiences and insights related to their patients receiving ICIs. To contextualize the information in a real-world manner, Nancy Taylor, ADN, a patient who is in ongoing treatment at the authors’ institution, gives her perspective of her experiences with the collaborative care team that has guided her though her ICI treatment. Included within the monograph are links to two patient-directed tools that APPs can download for their own use; these tools, along with resources for clinicians and patients, can be found in the Resources tab.
Overview of the Current Landscape
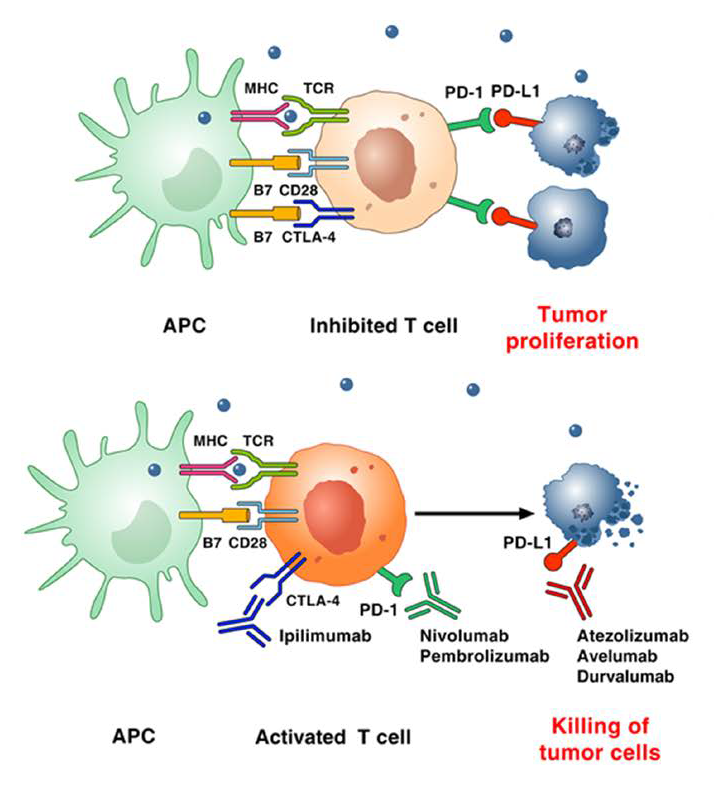
Immune checkpoints are cellular pathways important for the maintenance of self-tolerance and the prevention of indiscriminate attacks on healthy cells. In many cancer cells, immune checkpoint pathway activity is increased, allowing the cancer cells to grow unchecked by the body’s antitumor immune response. Inhibitors of these checkpoint pathways increase the body’s capacity to mount an immune response against cancer cells (Figure 1). Currently approved ICIs include monoclonal antibodies directed against cytotoxic T-lymphocyte–associated antigen 4 (CTLA-4), programmed cell death 1 (PD-1) protein, and programmed death ligand 1 (PD-L1) protein (Table 1 ).
Table 1. The treatment landscape of immune checkpoint inhibitors is changing rapidly. Please refer to the most recently published full prescribing information for each agent to view the most current list of approved indications.
Drug
Approved Indication
PD-1 inhibitors
Pembrolizumab
First line
Unresectable or metastatic melanoma
Metastatic nonsquamous NSCLC with no EGFR or ALK genomic tumor aberrations in combination with pemetrexed and platinum chemotherapy
Metastatic squamous NSCLC in combination with carboplatin and either paclitaxel or protein-bound paclitaxel
Stage III NSCLC with PD-L1 TPS ≥1% and no EGFR or ALK tumor aberrations in patients who are not candidates for surgical resection or definitive chemoradiation
Metastatic NSCLC with PD-L1 TPS ≥1% and no EGFR or ALK tumor aberrations
Locally advanced or metastatic UC in patients who are ineligible for cisplatin-containing chemotherapy and whose tumors express PD-L1 (CPS ≥10) or in patients who are not eligible for any platinum-containing chemotherapy regardless of PD-L1 status
Metastatic or unresectable, recurrent HNSCC in combination with platinum and 5-FU
Metastatic or unresectable, recurrent HNSCC with PD-L1 expression (CPS ≥1)
Recurrent locally advanced or metastatic MCC
Advanced RCC, in combination with axitinib
Second line
Metastatic NSCLC with PD-L1 TPS ≥1% and no EGFR or ALK genomic tumor aberrations with disease progression on or after platinum-containing chemotherapy
Metastatic NSCLC with PD-L1 TPS ≥1% and EGFR or ALK genomic tumor aberrations with disease progression on or after FDA-approved therapy for the genomic aberrations
Recurrent or metastatic HNSCC with disease progression on or after platinum-containing chemotherapy
Locally advanced or metastatic UC with disease progression during or following platinum-containing chemotherapy or within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy
Unresectable or metastatic, MSI-H or dMMR solid tumors that have progressed following prior treatment and who have no satisfactory alternative treatment options
Unresectable or metastatic, MSI-H or dMMR CRC that has progressed following treatment with a fluoropyrimidine, oxaliplatin, and irinotecan
Recurrent or metastatic cervical cancer with PD-L1 expression (CPS ≥1) with disease progression on or after chemotherapy
HCC after previous treatment with sorafenib
Third line
Metastatic SCLC with disease progression on or after platinum-based chemotherapy and at least one other prior line of therapy
Refractory PBMCL or relapsed PBMCL after 2 or more prior lines of therapy
Recurrent locally advanced or metastatic gastric or gastroesophageal junction adenocarcinoma with PD-L1 expression (CPS ≥1) with disease progression on or after ≥2 prior lines of therapy including fluoropyrimidine- and platinum-containing chemotherapy and if appropriate, HER2/neu-targeted therapy
Fourth line
Refractory cHL or relapsed cHL after 3 or more prior lines of therapy
Adjuvant therapy
Adjuvant treatment of melanoma with involvement of lymph nodes following complete resection
Nivolumab
First line
Unresectable or metastatic melanoma, as a single agent or in combination with ipilimumab
Intermediate or poor-risk, previously untreated advanced RCC, in combination with ipilimumab
Second line
Metastatic NSCLC with no EGFR or ALK mutations with disease progression on or after platinum-based chemotherapy or metastatic NSCLC with EGFR or ALK genomic tumor aberrations with disease progression after therapy for these mutations
Advanced RCC after prior anti-angiogenic therapy
cHL that has relapsed or progressed after autologous HSCT and brentuximab vedotin
Recurrent or metastatic HNSCC with disease progression on or after a platinum-based therapy
MSI-H or dMMR metastatic CRC that has progressed following treatment with a fluoropyrimidine, oxaliplatin, and irinotecan, as a single agent or in combination with ipilimumab
Locally advanced or metastatic UC with disease progression during or following platinum-containing chemotherapy
Locally advanced or metastatic UC with disease progression within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy
HCC previously treated with sorafenib
Third line
Metastatic SCLC with disease progression after platinum-based chemotherapy and ≥1 other lines of therapy
Fourth line
cHL that has relapsed or progressed after ≥3 lines of systemic therapy that includes autologous HSCT
Adjuvant therapy
Adjuvant treatment of melanoma with lymph node involvement or metastatic disease in patients who have undergone complete resection
Cemiplimab-rwlc
First line
Metastatic CSCC or locally advanced CSCC in patients who are not candidates for curative surgery or curative radiation
PD-L1 inhibitors
Atezolizumab
First line
Locally advanced or metastatic UC in patients who are not eligible for cisplatin-containing chemotherapy and whose tumors express PD-L1 (PD-L1-stained tumor-infiltrating IC covering ≥5% of the tumor area)
Locally advanced or metastatic UC in patients who are not eligible for any platinum-containing chemotherapy regardless of PD-L1 status
Metastatic non-squamous NSCLC with no EGFR or ALK genomic tumor aberrations, in combination with bevacizumab, paclitaxel, and carboplatin
Unresectable locally advanced or metastatic TNBC with PD-L1 expression (PD-L1-stained tumor-infiltrating IC covering ≥1% of the tumor area), in combination with protein-bound paclitaxel
Extensive-stage SCLC, in combination with carboplatin and etoposide
Second line
Locally advanced or metastatic UC with disease progression during or following any platinum-containing chemotherapy or within 12 months of neoadjuvant or adjuvant chemotherapy
Metastatic NSCLC with disease progression during or following platinum-containing chemotherapy (patients with EGFR or ALK genomic tumor aberrations should have disease progression on FDA-approved therapy for NSCLC harboring these aberrations prior to receiving atezolizumab)
Avelumab
First line
Metastatic MCC
Advanced RCC, in combination with axitinib
Second line
Locally advanced or metastatic UC with disease progression during or following platinum-containing chemotherapy
Locally advanced or metastatic UC with disease progression within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy
Durvalumab
Second line
Locally advanced or metastatic UC who have disease progression during or following platinum-containing chemotherapy
Locally advanced or metastatic UC who have disease progression within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy
Consolidation therapy
Unresectable stage III NSCLC without disease progression following definitive concurrent platinum-based chemoradiation
CTLA-4 inhibitor
Ipilimumab
First line
Unresectable or metastatic melanoma, as a single agent or in combination with nivolumab
Intermediate- or poor-risk, previously untreated advanced RCC, in combination with nivolumab
Second line
MSI-H or dMMR metastatic CRC that has progressed following treatment with a fluoropyrimidine, oxaliplatin, and irinotecan, in combination with nivolumab
Adjuvant therapy
Adjuvant treatment for cutaneous melanoma with pathologic involvement of regional lymph nodes of >1 mm following complete resection, including total lymphadenectomy
Note. There is an ever-expanding list of approved indications for current ICIs. Please refer to the most recently published full prescribing information for each agent to view the most current list of approved indications. ALK = anaplastic lymphoma kinase; cHL = classical Hodgkin lymphoma; CPS = combined positive score; CRC = colorectal cancer; CSCC = cutaneous squamous cell carcinoma; dMMR = mismatch repair-deficient; EGFR = epidermal growth factor receptor; HCC = hepatocellular carcinoma; HNSCC = head and neck squamous cell carcinoma; HSCT = hematopoietic stem cell transplantation; IC= immune cells; MCC = Merkel cell carcinoma; MSI-H = microsatellite instability-high; NSCLC = non–small cell lung cancer; PMBCL = primary mediastinal large B-cell lymphoma; RCC = renal cell carcinoma; SCLC = small cell lung cancer; TNBC = triple-negative breast cancer; TPS = tumor proportion score; UC = urothelial carcinoma of the bladder. Information from AstraZeneca Pharmaceuticals LP (2018); Bristol-Myers Squibb Company (2019a, 2019b); EMD Serono, Inc., & Pfizer, Inc. (2019); Genentech, Inc. (2019); Merck & Co. (2019); Regeneron Pharmaceuticals, Inc. (2019).
Figure 1. Checkpoint inhibitor mechanism of action. APC = antigen presenting cell. Adapted, with permission, from Circulation (Varricchi et al., 2017).
Though each of these therapies was initially tested in one disease, ICIs are now used in multiple tumor types, including both solid and hematologic malignancies. Importantly, treatment benefit is independent of age, and patients with autoimmune disease may still benefit. Thus, agents are being used in an increasing number of patients in both academic and community settings, and many of these patients are managed by APPs. In addition to their use as single agents, ICIs are also being tested and approved for use in combination with other ICIs, cytotoxic therapies, small molecules, and radiotherapy.
For which of the following solid tumors do you have the most clinical experience using ICIs.
Several ICIs are currently being evaluated in clinical trials. Some of the ICIs under study have novel mechanisms of action, while other studies are focused on additional indications for already approved agents or combination therapy with other agents. For example, agents targeting PD-1, PD-L1, and CTLA-4 are in phase III and IV clinical trials in several types of cancers, including head and neck, renal cell, gastric, hepatocellular, lung, urothelial, and ovarian cancers; melanoma; non-Hodgkin lymphoma and multiple myeloma; and others (ClinicalTrials.gov, 2019; Darvin, Toor, Sasidharan Nair, & Elkord, 2018).
In addition, other immune checkpoint therapies are in various stages of clinical development. These therapies include agents that target inhibitory immune checkpoint lymphocyte activation gene-3 (LAG-3; Long et al., 2018), T-cell immunoglobulin and mucin domain 3 (TIM-3; Xia et al., 2018), V-domain immunoglobulin-containing suppressor of T-cell activation (VISTA; Linhares, 2018), human endogenous retrovirus-H long terminal repeat-association protein 2 (HHLA2) immunostimulants (Shimonosono et al., 2018), tumor necrosis factor receptor OX40, and glucocorticoid-induced tumor necrosis factor-related (GITR) immunostimulants (Schoenhals et al., 2018).
With which of the following tumor types do you have the least experience?
Challenges in Monitoring for irAEs in the Clinic
The same mechanisms responsible for the efficacy of ICIs are responsible for their toxicities. Immune checkpoint inhibitor activation of autoreactive T cells gives rise to a unique constellation of irAEs. Because ICIs increase immune activity throughout the body, irAEs can occur in any number of organ systems due to inflammation. When considering patient safety and optimal management of irAEs, there are a number of factors to evaluate. First, ICIs have been brought to market much faster than many other cancer therapies. All currently approved therapies obtained expedited approval for at least one indication. Of note, post-approval modifications to drug labels are common in cancer therapies, especially for drugs that are approved for indications without the benefit of robust supporting randomized clinical trial data, as are generally available for approved agents (Shepshelovich et al., 2018). Second, the number of cancers that can be treated with these drugs introduces variability in the expected pattern of irAEs, as the patient’s underlying condition may drive irAE incidence or severity (e.g., pneumonitis in lung cancer).
Yet another source of variability in the expected pattern of irAEs is introduced by the real-world patient population. Characteristics of patient populations are tightly controlled in clinical studies. As ICI use grows in the clinic, a broader range of patients, some of whom may have inflammatory comorbid conditions such as autoimmune diseases or diabetes, can receive treatment. This introduces potential variation in irAE patterns that must be accounted for by APPs and the whole collaborative practice team; rigorous monitoring and management approaches are essential.
Compounding the issues presented by a growing number of indications and patient population variability is the emergence of combination therapy regimens and long-term, and in some cases lifelong, use of treatments.
How confident are you that your patients treated with ICIs are effectively monitoring for and reporting irAEs?
With the above factors at play, making generalizations can be challenging. With the growing complexity of care, there may be unique challenges for APPs in community practice, who must evaluate and interpret emerging evidence and best practices across a wide range of malignancies. It is critical that APPs work with their treatment teams to ensure diligent monitoring for irAEs throughout the patient’s treatment and indefinitely after.
Advanced practice providers can help improve patient outcomes by empowering their patients to take an active role in the early identification of irAEs through the provision of decision tools and patient-centered strategies that facilitate early identification and monitoring of irAEs. This important concept will be revisited later on in the monograph and in the accompanying videos.
Characteristics of irAEs
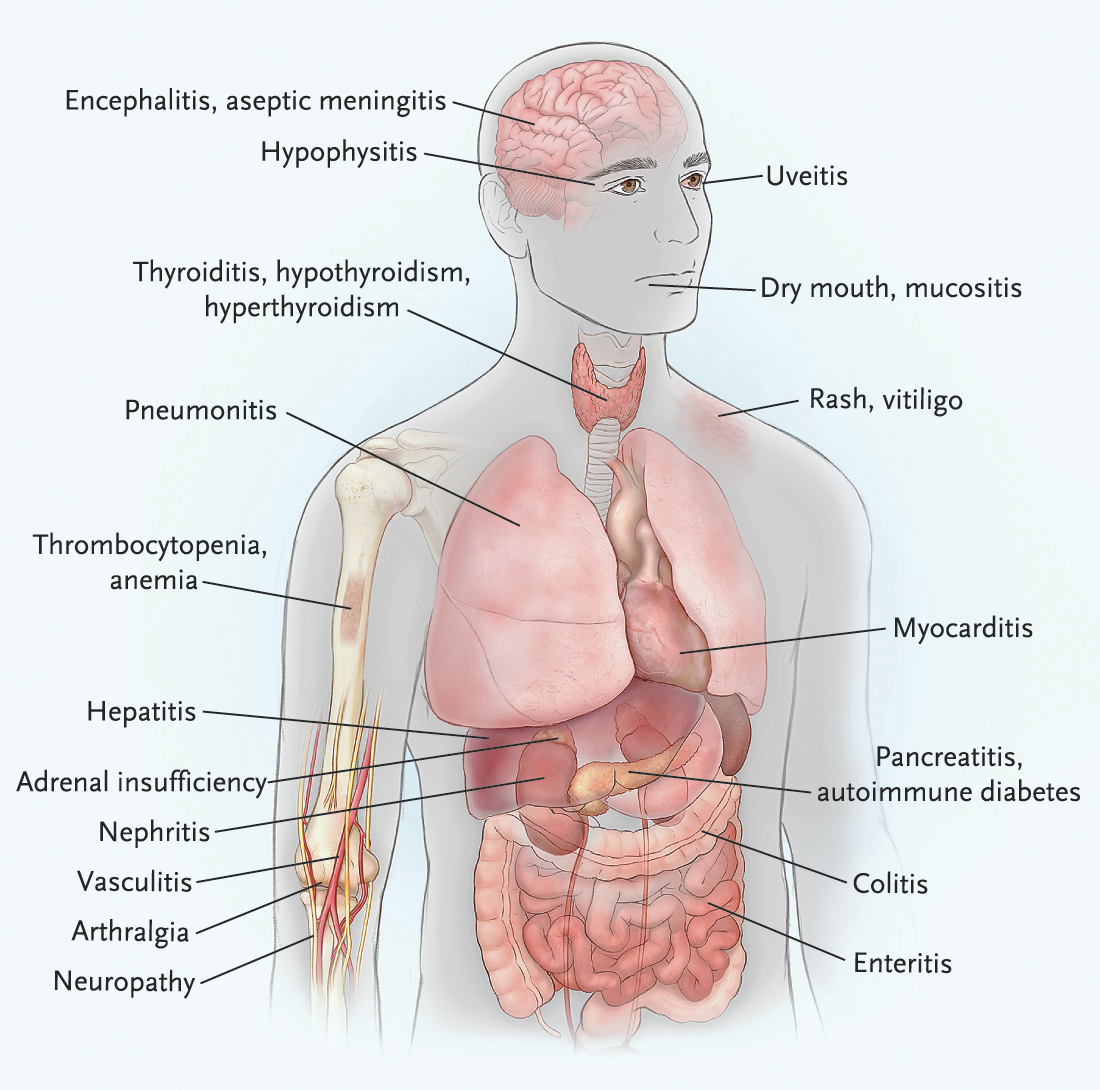
As with cytotoxic agents, checkpoint inhibitors can give rise to AEs in a number of organ systems. The risk factors for irAEs are unclear, and it is unknown why some patients experience AEs when others do not (Postow, Sidlow, & Hellmann, 2018). The systemic nature of checkpoint inhibition means that any of the body systems can become inflamed (Figure 2).
Figure 2. Immune checkpoint blockade can result in inflammation of any organ. Shown are the most common irAEs that clinicians encounter in patients treated with immune checkpoint blockade. Reproduced, with permission, from The New England Journal of Medicine (Postow et al., 2018).
Though a large majority of patients treated with either cytotoxic chemotherapy or ICIs will experience mild AEs such as diarrhea, fatigue, nausea, and decreased appetite (Seidel, Otsuka, & Kabashima, 2018), AEs such as anemia, neutropenia, alopecia, myalgia, and stomatitis are largely restricted to cytotoxic chemotherapy. On the other hand, pruritus, rash, hypothyroidism, and pneumonitis are AEs characteristic of ICIs (Khan et al., 2018). More severe side effects of ICIs include severe diarrhea, colitis, increased alanine aminotransferase levels, inflammation pneumonitis, and interstitial nephritis (Seidel et al., 2018). In addition, the increased overall inflammation can cause autoimmune conditions to worsen, or even prompt emergence of inflammatory conditions such as type 1 diabetes mellitus.
Though each agent has shown safety profiles that vary between indications and studies, overall, pneumonitis is more common with PD-1 and PD-L1 checkpoint inhibitors, and colitis and hypophysitis are more common with CTLA-4 checkpoint inhibitors. While the frequency of colitis reported in the literature ranges from 8% to 27%, the incidence of diarrhea is as high as 54% in patients treated with anti–CTLA-4 antibodies, especially in those who receive anti–CTLA-4 and anti–PD-1 combination therapy (Xu et al., 2018). Clinical trials that have compared ICI AE profiles have shown that more patients experienced side effects when treated with an anti-CTLA-4 agent (27.3%) than with an anti-PD-1 agent (16.3%). Importantly, more patients experienced an irAE when treated with a combination of ICIs (55%; Seidel et al., 2018).
Timing and Severity
Adverse events can range in severity, but in all cases, early identification is particularly important. Most often, symptoms are initially low grade in severity and can be managed while therapy is maintained. If left untreated, irAEs can evolve into serious and life-threatening complications that can prompt a more sustained interruption (and sometimes permanent discontinuation) in therapy. Immune-related AEs may also result in permanent, lifelong conditions, and full organ function may not recover even if the ICI is discontinued. For example, patients who develop hypothyroidism may require lifelong hormone replacement therapy.
Case SpotlightA gentleman with UC was receiving ICI therapy. He was a very active man, working full time in a construction job, and had been able to continue working during his treatment initiation. Fortunately, scans showed he was having an excellent response to therapy. At week 12, he reported a significant increase in fatigue over the course of several days. He had not been able to work for the preceding 2 days, needing to take short naps during the day. His APP reviewed his vital signs (stable), complete blood count (within normal limits [WNL]), and complete metabolic panel (WNL). She ordered a thyroid panel (thyroid-stimulating hormone [TSH] with free T4) and found that his TSH level had increased to 18 mU/L. Free T4 was at the lower end of normal range. The APP diagnosed the patient with hypothyroidism, and he was started on levothyroxine at 1.6 µg/kg/day. Within several days the patient’s energy level improved and he was able to return to work the following week. This case illustrates the importance of early identification of irAEs.
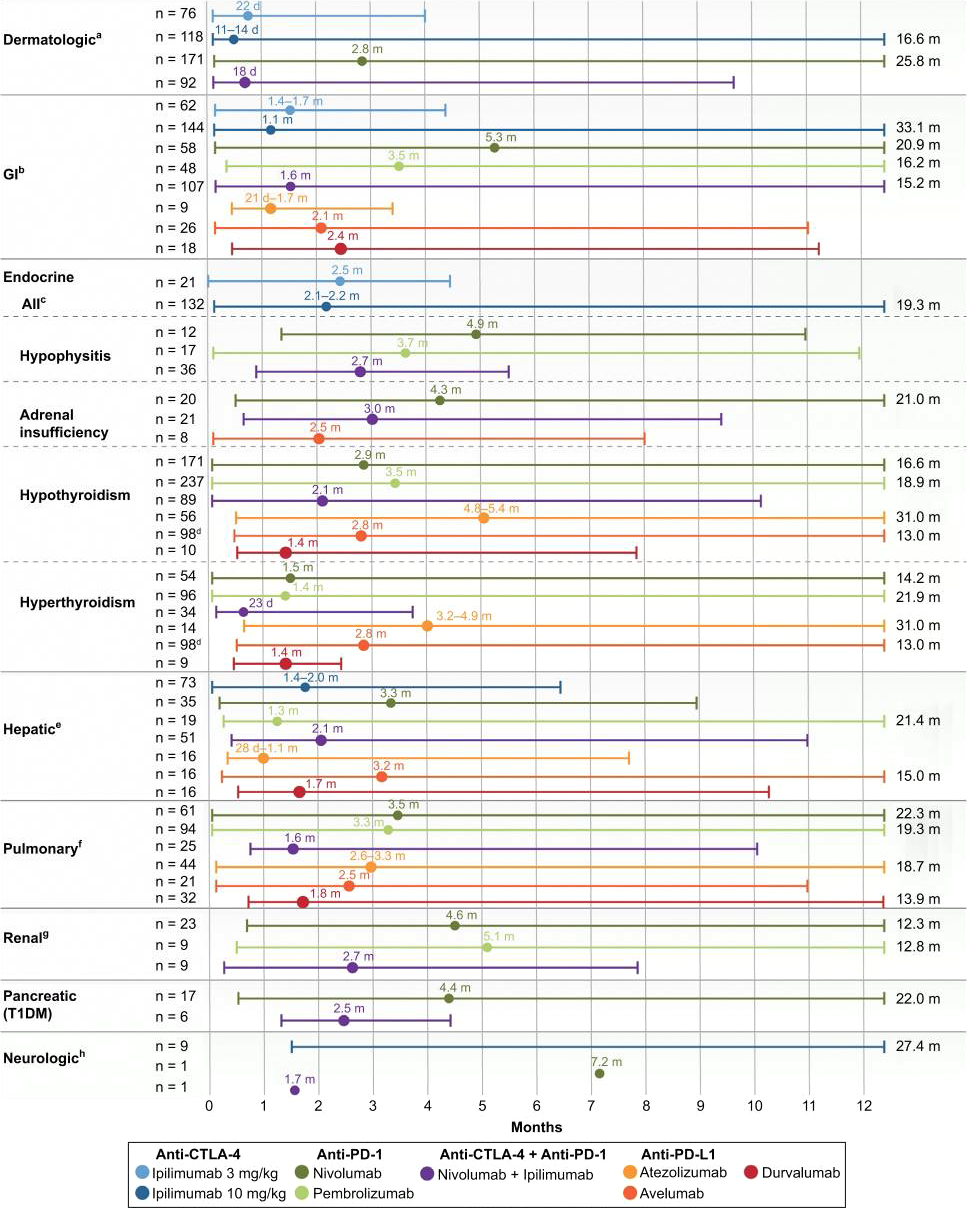
Immune-related AEs can occur at any time during treatment, from days to months after administration of an ICI, and even after therapy has been discontinued. Figure 3 illustrates a common pattern for timing, in which irAEs emerge primarily within a period of weeks to months following treatment initiation. However, this pattern is seen with single-agent ICIs; variability may exist with combination ICIs and ICIs plus cytotoxic chemotherapy. Further, the timing and impact on different organ systems can vary between individuals and between tumor types. Early identification is particularly important because most symptoms are generally low-grade when detected early.
The duration of FDA-approved therapies varies, and evidence regarding how irAEs arise in the context of long-term survivorship is still growing. Because of the potential for delayed onset, monitoring should be included in the patient’s survivorship plan.
Figure 3. Time to onset of immune-mediated toxicities (median and range). Reprinted, with permission, from ImmunoTargets and Therapy (Davies & Duffield, 2017).
ICIs in Combination
It is critical not to underestimate the amplified risk of irAEs in the context of combined ICIs and ICIs plus adjuvant therapy (Davies & Duffield, 2017). This is a growing issue, as a durable response is achievable with monotherapy in only a small subset of patients (~25% of patients; Marin-Acevedo et al., 2018). The incidence and severity of irAEs associated with individual agents can worsen in the context of combination therapy, and the timing and pattern of emergence is altered. When combining ICIs, no symptoms unique to the combination have been noted, but there is an increased rate of occurrence and intensity. A higher percentage of patients experience irAEs, and irAEs are more likely to be grade 3 or 4 than if the agents are used in isolation (Wolchok et al., 2017). Because irAEs in combination therapy are generally of a higher grade, monitoring is of particular importance in this context (Boutros et al., 2016; Davies & Duffield, 2017; Hassel et al., 2017).
Management of irAEs
To date, there have been no controlled trials aimed at identifying the optimal treatment for irAEs, and practice guidelines are based on consensus among clinical experts. Identifying the cause of a given symptom as related to an irAE can be confounding, given that such symptoms often overlap those due to a variety of other causes (i.e., comorbid conditions, other cancer therapies, disease complications). As such, irAEs are often diagnoses of exclusion. With a growing evidence base showing improved response rates in multiple disease sites with combination ICI and chemotherapy, tyrosine kinase inhibitors, hormonal therapy, and radiation therapy, identifying the root cause of AEs becomes more of a challenge for APPs and the entire treatment team.
For this reason, it is important to be systematic in identifying and treating emerging symptoms. In the management of irAEs, relationships with subspecialists well educated on the spectrum of irAEs can improve outcomes. Several sets of guidelines have been developed based on the consensus of expert clinicians, predominantly from academic research facilities. Such guidelines should serve as a guide to clinicians in the community who are new to ICI therapy. As the breadth of knowledge and experience grow, the guidelines are revised to reflect the collective experiences of clinicians familiar with ICI treatment and irAEs.
Guidelines
Specific strategies for the management of toxicities have been developed and recommended by national professional organizations. These serve as a resource for APPs and members of the entire collaborative care team to guide specific management.
Guidelines from the National Comprehensive Cancer Network (NCCN, 2019), the American Society of Clinical Oncology (Brahmer et al., 2018), the Society for Immunotherapy of Cancer (SITC; Puzanov et al., 2017), and the European Society for Medical Oncology (Haanen et al., 2017) are helpful for ruling out comorbid medical events that can give rise to symptoms that can be mistaken for irAEs, as well as suggesting strategies to be used in the differential diagnosis. Once an event is determined to be an irAE, the guidelines provide appropriate interventions based on the grade and/or severity of the event.
Which of the following irAEs have you encountered most often?
Though guidelines form a strong foundation for management, they are by no means exhaustive, and open questions remain surrounding irAE management. Efforts are underway to explore strategies to preempt the onset of toxicities, as well as to evaluate the sequencing and timing of immunosuppressant therapy. Advanced practice providers should be vigilant in watching for new data and guidelines relevant to management of irAEs and be prepared to evaluate and integrate them into practice proactively.
Grading
When applying these guidelines, it is important that grading criteria from the Common Terminology Criteria for Adverse Events (U.S. Department of Health and Human Services, 2018) be used to ensure consistency in communication and management. These criteria can also be used to grade toxicity occurring during multimodal treatment, and they are commonly used to guide clinical care decisions. The current CTCAE was developed based on contemporary knowledge and experience with cytotoxic therapies. The criteria are undergoing revisions to incorporate information that more closely reflects AEs associated with ICI therapy.
It is important to monitor for irAEs throughout and following treatment. In general, if an irAE is identified when it is low grade, treatment with ICI therapy may continue. For grade 2 irAEs, ICI treatment is interrupted, and immunosuppressant intervention should be considered. For grade 3 and 4 toxicity, ICI discontinuation will most often be recommended with initiation of immunosuppressant therapy.
Immunosuppressant Therapy
In most cases, immunosuppression is used to reduce symptom-causing inflammation. Glucocorticoids are frequently used as first-line immunosuppressive agents, and additional medications can be added if the irAE is refractory to the first line of immunosuppression (NCCN, 2019). Patients often experience rapid improvement of symptoms when an appropriate steroid dose is administered. If a patient does not have rapid relief of symptoms, another cause for the symptoms of the suspected irAE should be considered.
Once an irAE is identified and management measures are initiated, it is important for the APP to ensure that patients understand that steroids are given until the irAE resolves and then are tapered. Patients should also be aware of the AEs associated with steroids and encouraged to contact the oncologist’s office if the symptoms become troublesome. In addition, APPs must educate patients that it is important to continue taking the steroids until instructed by their oncology provider that they can stop, as doing otherwise can lead to inflammatory symptoms.
Case SpotlightA patient on ICI therapy who developed grade 2 pneumonitis was started on a dose of prednisone of 1 mg/kg/day. As she weighed 58 kg, the dose was 60 mg/day. Her symptoms of shortness of breath and cough improved in 5 days. Her oxygen saturation stabilized, yet it did not return to baseline. She continued on the 60-mg/day dose until week 2, at which time oxygen levels improved to baseline. At this point, the steroid taper was started with reduction of dosing by 10 mg every week. A follow-up CT scan confirmed improvement in ground-glass opacities. Once the steroids were tapered off, the team discussed with the patient that as she was grade 2, they could rechallenge with the ICI, yet there would be a risk for recurrence. After an informed discussion, the decision was to rechallenge, with very close monitoring. This case illustrates how appropriate management of an irAE with steroids can preserve the opportunity for treatment continuation.
Glucocorticoid immunosuppression is associated with potential AEs such as hyperglycemia, edema, anxiety, gastritis, and adrenal insufficiency. Further, glucocorticoid use presents an additional risk of opportunistic infection, and long-term use can lead to osteoporosis. Practicing clinicians must monitor for these potential side effects; for example, patients should have blood glucose levels monitored regularly. Patients should be educated to take the steroid with food, and a proton pump inhibitor or H2 blocker should be prescribed to reduce the risk of gastritis. An antibiotic, such as sulfamethoxazole/trimethoprim, should be prescribed to reduce the risk of Pneumocystis jirovecii pneumonia. If the patient has a known sulfa allergy, an alternative antibiotic should be substituted. After resolution of the irAE, steroids must be tapered slowly over the course of weeks in order to avoid risk of flare of inflammatory side effects (NCCN, 2019).
In some cases, the irAE being experienced by the patient may be refractory to the initial management strategy (use of steroids). If the irAE is not responsive or progresses, additional immunosuppressant agents may be required. The use of these agents is extrapolated from use in autoimmune conditions. Additional immunosuppressant therapies include infliximab, mycophenylate mofetil, IV immunoglobulin, disease-modifying antirheumatic agents, and others. For instance, infliximab may be used to treat colitis. It is important to note that infliximab is contraindicated in cases of hepatitis, as it may lead to reactivation of viruses such as HBV and HCV. Mycophenylate mofetil is recommended in the treatment of hepatitis (Brahmer et al., 2018; NCCN, 2019; Puzanov et al., 2017).
Current understanding of the mechanism of irAEs is incomplete, but there does not appear to be a connection between the emergence of inflammatory AEs and treatment efficacy. Importantly, treatment benefit can persist in patients on immunosuppressive therapy, and clinical outcomes are similar in patients who do not require intervention for irAEs and those who do require immunosuppressive therapy (Postow et al., 2018).
Impact of Comorbidities
As therapies move from the tightly controlled populations recruited for clinical trials to the real
world, irAEs occur in patients with a range of comorbid conditions not included in clinical trials.
The identification of emergent symptoms may be more difficult for patients in the context of other issues. In addition, comorbid conditions further compound the challenge of identifying the cause of AEs that surface during treatment with combination therapy. In cases when patients have comorbidities, the use of journaling and symptom tracking, and communication between clinicians become even more important, and patients should be given instructions to contact the office when experiencing shifts from baseline.
Case SpotlightA patient with multiple sclerosis (MS) was diagnosed with metastatic melanoma. She was presented with several treatment options that included ICI therapy. Her APP worked to ensure that the patient understood the risk of MS flare or worsening. After discussing options with her family and the members of the care team, she elected to proceed with ICI therapy. She did have an MS flare, but she also had a significant response to therapy. After completion of ICI therapy, her melanoma is in remission. She has residual reduced ambulatory ability, requiring use of a leg brace and a crutch. This case illustrates the importance of patient education and awareness, as well as shared decision-making, in achieving the best possible outcomes in the setting of ICI treatment and a significant comorbidity.
Monitoring Strategies
Clinician Monitoring
Ideally, a patient experiencing an AE is managed by an oncology specialist. Because ICI therapies are new, general practitioners and primary care physicians may not be aware of the full spectrum of toxicities, and the signs/symptoms of irAEs can mimic other medical conditions. As such, the oncology team is best prepared to conduct the differential diagnosis. Referral to and treatment by oncology specialists is imperative to provide potentially life-saving management, as the treatment of irAEs can differ drastically from the treatment of other conditions that present similarly.
Regardless of setting, every effort should be made to diligently monitor patients for irAEs as they emerge. An effective twofold approach includes the use of in-office processes and procedures (e.g., telephone triage) that keep communication lines open, plus the use of tools (e.g., decision aides, electronic medical record) that prompt timely communication with the patient’s oncology team from other clinicians, caregivers, and the patient him/herself.
In the current oncology arena, it is a rare practice that does not employ a collaborative practice model. In some oncology offices, there is a dedicated nurse or staff member assigned to telephone triage when patients contact the office to report irAE symptoms. In other offices, the staff may share the responsibility. In these instances, the nurse or staff member must have the clinical experience to understand the nature and severity of patient symptoms and how they may be managed. All professionals and para-professionals within the office must be educated on triage guidelines and deliver consistent messaging and instructions to patients. It is essential that staff members immediately recognize when a patient requires immediate assessment and intervention.
Case SpotlightA patient with lung cancer currently being treated with ICI therapy called in to the mid-sized community oncology office where her care team practiced to cancel her standing appointment, stating that she had an upper respiratory infection (URI). She reported that it had developed over the weekend, and that she had gone to a walk-in clinic. She was prescribed an antibiotic, which she began taking. The patient clearly believed that her URI was just an ordinary occurrence that was of no particular consequence. The practice nurse who was triaging the phone call asked the additional questions about associated symptoms that she had been trained to ask: “Do you have a fever? Do you have a cough? Are you short of breath?” The patient answered that she did not have a fever, but that she did have a new non-productive cough and was indeed short of breath. The practice nurse notified the APP immediately. Both clinicians recognized that this could potentially be pneumonitis and not a bacterial/viral URI. It was essential for the patient to come in to clinic for evaluation. The practice nurse instructed the patient to come in. Upon her arrival, her vital signs were assessed, and it was noted that her oxygen saturation was lower than previous measurements and dropped upon ambulation. There were no other data to support an infection. The APP ordered a CT scan for evaluation. The scan confirmed new ground-glass opacities, and the patient was diagnosed with pneumonitis, an irAE. As she was symptomatic and had diagnostic changes, this was grade 2 according to the CTCAE. The patient’s ICI therapy was held, and she was started on prednisone promptly, and she eventually was able to be rechallenged with ICI therapy. This case illustrates the importance of training all office staff in thorough and productive patient questioning.
Patient Awareness and Self-Monitoring
Making sure that patients are aware of AEs that may occur is of the utmost importance. In particular, it is crucial for APPs to be sure their patients understand the importance of reporting changes from baseline in terms of ease of breathing, fatigue, and increase in diarrhea immediately. APPs should use straightforward language to ensure that patients understand the symptoms that must be reported. Because patients may avoid contacting the office, either in an attempt not to “bother” the office or to avoid “complaining,” reinforcing the importance of communicating key symptoms should be presented to patients at every single visit. Every staff member who comes in contact with the patient should take the opportunity to remind patients that their calls are encouraged and never a bother.
A common obstacle to irAE reporting by patients is the fear that if they experience an irAE, they will have to stop treatment. This anxiety is particularly pronounced in patients in a clinical trial who may have exhausted other treatment options. In discussing reporting with patients, it is critical that APPs convey the fact that irAEs do not necessarily mean they will have to discontinue treatment, and in some cases, a treatment discontinuation may not be permanent. If untreated, some irAEs can cause significant damage to the body’s organ systems and can limit the number of other viable treatment options. It is important to emphasize that irAEs can worsen, and that it is most helpful for patients to inform the care team of irAEs.
Though lists of symptoms are helpful for patients to recognize irAEs, an overarching message for APPs to convey to patients is that changes from baseline are important. For example, an increase in fatigue may be a normal adverse event, or it may be a sign of endocrine issues. Emphasizing that patients should report all changes can help patients understand when they should call the office.
Monitoring must extend beyond in-office contact with the patient and exist as part of the patient’s daily life to achieve the most efficient irAE monitoring. Giving patients tools for at-home monitoring and documenting of symptoms of potential irAEs can facilitate early detection of irAEs and increase the likelihood that they can be managed before a visit to an emergency department is required or before treatment interruption is necessary. A diary or tracking tool can help make sure that newly emerging symptoms are not ignored or compartmentalized as a “new normal” for the patient (Hermansen-Kobulnicky & Purtzer, 2014).
How often do you distribute an irAE symptom checklist during the first visit with a patient being prescribed ICI therapy?
Patients may benefit from receiving a checklist of clinical situations to prompt them to contact the office or to be evaluated. This checklist can serve to remind both caregivers and patients of the most common irAE symptoms, as well as provide a reference of less common symptoms that should prompt communication with the office. Inclusion of specific instructions for communication with the office staff can help ensure that irAEs are flagged as such and communicated immediately to the appropriate clinician. Patients should be encouraged to adopt the habit of daily symptom self-assessment, even if they do not believe they are feeling anything amiss.
Patient journaling, whether on paper or with a digital tool, has been shown to improve both patient-clinician communication and symptom management (Hermansen-Kobulnicky & Purtzer, 2014). For example, daily tracking of symptoms can assist in the grading of a toxicity. Further, including caretakers in the process of tracking symptoms can also help them feel empowered and valued as a care partner. Beyond the basic practice of recording symptoms, the act of journaling has been shown to improve awareness of sensations and patterns of daily activity. The act of writing down each day’s happenings improves awareness beyond what can be accomplished through diligence alone.
Case SpotlightA patient who was diligent about journaling daily symptoms, activities, and nutritional intake was most concerned about nutrition. She was most interested in discussing nutrition during her office visits. Over the course of 2 weeks, however, her journal revealed that she was walking increasingly shorter distances. When questioned by her AP, the patient was not aware of this decrease; she could only recall being “more tired.” The data in the journal helped prompt a more detailed workup. The patient was found to have decreased exercise capacity due to an emerging pneumonitis. This was confirmed by monitoring oxygen saturation and results of a CT scan. She was treated by holding ICI therapy and a course of steroids. Once pneumonitis was resolved, the patient successfully continued treatment. Though this case illustrates the importance of journaling for identifying irAEs, it is also important to note that daily tracking of symptoms can assist in the grading of the toxicity.
In addition to providing a journal for tracking symptoms, following up with high-risk patients—whether the increased risk is due to lack of family support, low literacy/numeracy, or a complex clinical situation—via a post-treatment phone call can help to identify early treatment issues and serve as a reminder that contact with the oncologist’s office is a welcomed and important part of care.
Communicating With Clinicians Outside the Oncology Office
To promote communication between clinicians in instances in which the patient must receive care outside of his or her oncologist’s office, such as while traveling or in an emergency situation, patients can be encouraged to carry a personalized medication card to present to the treating medical staff. The card ensures that the provider is aware of the patient’s ongoing treatment with an ICI. Having the card allows the patient to communicate medically accurate information with confidence to a new clinician, thereby encouraging communication between the patient, the oncology office, and the provider outside of the oncology office.
How often do you distribute an irAE symptoms checklist at every patient visit for a patient who is taking an ICI?
This information provides treating clinicians with the facts they need to provide the most appropriate intervention for the patient. In addition to the list of medications, the card should contain the patient’s diagnosis and contact information for the oncologist’s office. Instructions should be provided for the treating clinician to immediately contact the covering oncology team.
The medication card is an especially powerful tool for patients receiving off-site care in a location geographically distant from their oncologist’s office, or in situations where the electronic medical record (EMR) is separate from the EMR at the oncology provider’s office. In addition, a large facility with many specialties within the system may place a “flag” or an “alert” on a chart so that providers in other departments are aware of the patient’s current treatment regimen.
Conclusions
As the use of ICIs continues to expand in clinical practice, it is critical that APPs be able to identify and manage the associated irAEs. This is particularly true in many community practices, where APPs and their collaborative team members manage patients with a wide variety of malignancies and perhaps have fewer opportunities for on-site education regarding the safe and effective administration of ICIs. Adverse events seen in the setting of ICI therapy can vary with respect to severity, organ system affected, and timing. With proper management, however, most patients can continue their therapy once the AE has been treated and the issue has been resolved. Understanding the characteristic presentation of common irAEs, such as pneumonitis and colitis, as well as the presentation of less common irAEs can facilitate early irAE identification in the context of combination therapy.
The ability to interpret and integrate into patient care the best practices endorsed by society guidelines regarding grading and treating irAEs in a timely manner is critical for APPs. In addition, they must be sure to monitor for updated guideline recommendations and other emerging evidence to be sure they are providing the best care to effect optimal patient outcomes.
Advanced practice providers should have at their disposal effective strategies to engage patients in their own care and irAE monitoring. Processes that empower patients to report AEs early can include provision of a list of symptoms that should prompt patients to contact the office, provision of a medication card that can facilitate communication with acute care physicians, and clinician review of patient journals during office visits, among other strategies.
Optimal patient self-monitoring and communication with the oncology team are crucial elements that must be in place to ensure safe and effective administration of ICI therapy. But APPs and every member of the treatment team and office staff must work together to be sure patients have the education, tools, and level of comfort they need to best monitor and advance their own health.
Clinical Pearls
Immune-related AEs can occur in any body system where inflammation can occur. A high level of suspicion that the AE is treatment related should be maintained.
The timing of irAEs is variable. They can occur at any time during the course of treatment, as well as at any point following the cessation of therapy.
Though use of combination therapy with multiple ICIs and with other types of agents can alter the AE profile, intensity is often increased.
Advanced practice providers should be vigilant in watching for emerging evidence and guideline updates relevant to the management of irAEs and be prepared to interpret and integrate them into practice proactively.
Diligence in monitoring for irAEs is critically important because when treated early, they are often manageable and need not limit continuation of therapy.
Advanced practice providers must educate patients that changes from baseline in areas such as ease of breathing, fatigue, and increase in diarrhea must be reported to the office immediately. Patients should be given the tools and resources they need to monitor their own symptoms at home between visits.
It is the job of every member of the collaborative practice team to reinforce the message that patients should monitor their symptoms and contact the office when changes arise.
Boutros, C., Tarhini, A., Routier, E., Lambotte, O., Ladurie, F. L., Carbonnel, F.,...Robert, C. (2016). Safety profiles of anti-CTLA-4 and anti-PD-1 antibodies alone and in combination. Nature Reviews Clinical Oncology, 13(8), 473-486. https://doi.org/10.1038/nrclinonc.2016.58
Brahmer, J. R., Lacchetti, C., Schneider, B. J., Atkins, M. B., Brassil, K. J., Caterino, J. M.,…Thompson, J. A. (2018). Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American Society of Clinical Oncology Clinical Practice Guideline. Journal of Clinical Oncology, 36(17), 1714-1768. http://dx.doi.org/10.1200/JCO.2017.77.6385
Darvin, P., Toor, S. M., Sasidharan Nair, V., & Elkord E. (2018). Immune checkpoint inhibitors: Recent progress and potential biomarkers. Experimental & Molecular Medicine, 50(12), 165. https://dx.doi.org/10.1038/s12276-018-0191-1
Davies, M., & Duffield, E. A. (2017). Safety of checkpoint inhibitors for cancer treatment: Strategies for patient monitoring and management of immune-mediated adverse events. ImmunoTargets and Therapy, 6, 51-71. https://doi.org/10.2147/ITT.S141577
Haanen, J., Carbonnel, F., Robert, C., Kerr, K., Peters, S., Larkin, J., & Jordan, K. (2017). Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of Oncology, 28(suppl 4), iv119-iv142. https://doi.org/10.1093/annonc/mdx225
Hassel, J. C., Heinzerling, L., Aberle, J., Bahr, O., Eigentler, T. K., Grimm, M. O.,...Gutzmer, R. (2017). Combined immune checkpoint blockade (anti-PD-1/anti-CTLA-4): Evaluation and management of adverse drug reactions. Cancer Treatment Reviews, 57, 36-49. https://doi.org/10.1016/j.ctrv.2017.05.003
Hermansen-Kobulnicky, C. J., & Purtzer, M. A. (2014). Tracking and journaling the cancer journey. Clinical Journal of Oncology Nursing, 18(4), 388-391. http://dx.doi.org/10.1188/14.CJON.388-391
Khan, M., Lin, J., Liao, G., Tian, Y., Li, R., Liu, M., & Yuan, Y. (2018). Comparative analysis of immune checkpoint inhibitors and chemotherapy in the treatment of advanced non-small cell lung cancer: A meta-analysis of randomized controlled trials. Medicine (Baltimore), 97(33), e11936. http://dx.doi.org/10.1097/MD.0000000000011936
Linhares, A. D. S., Leitner, J., Grabmeier-Pfistershammer, K., & Steinberger, P. (2018). Not all immune checkpoints are created equal. Frontiers in Immunology, 31 August. https://dx.doi.org/10.3389/fimmu.2018.01909
Long, L., Zhang, X., Chen, F., Pan, Q., Phiphatwatchara, P., Zeng, Y., & Chen, H. (2018). The promising immune checkpoint LAG-3: From tumor microenvironment to cancer immunotherapy. Genes Cancer, 9(5-6), 176-189. https://dx.doi.org/10.18632/genesandcancer.180
Marin-Acevedo, J. A., Dholaria, B., Soyano, A. E., Knutson, K. L., Chumsri, S., & Lou, Y. (2018). Next generation of immune checkpoint therapy in cancer: New developments and challenges. Journal of Hematology and Oncology, 11(1), 39. https://dx.doi.org/10.1186/s13045-018-0582-8
Postow, M. A., Sidlow, R., & Hellmann, M. D. (2018). Immune-related adverse events associated with immune checkpoint blockade. New England Journal of Medicine, 378(2), 158-168. https://dx.doi.org/10.1056/NEJMra17033481
Puzanov, I., Diab, A., Abdallah, K., Bingham, C. O. 3rd, Brogdon, C., Dadu, R.,…Ernstoff, M. S. (2017). Managing toxicities associated with immune checkpoint inhibitors: Consensus recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group. Journal for Immunotherapy of Cancer, 5(1), 95. https://dx.doi.org/10.1186/s40425-017-0300-z
Schoenhals, J. E., Cushman, T. R., Barsoumian, H. B., Li, A., Cadena, A. P., Niknam, S.,…Welsh, J. W. (2018) Anti-glucocorticoid-induced tumor necrosis factor–related protein (GITR) therapy overcomes radiation-induced Treg immunosuppression and drives abscopal effects. Frontiers in Immunology, 9, 2170. https://dx.doi.org/10.3389/fimmu.2018.02170
Seidel, J. A., Otsuka, A., & Kabashima, K. (2018). Anti-PD-1 and anti-CTLA-4 therapies in cancer: mechanisms of action, efficacy, and limitations. Frontiers in Oncology, 8, 86. https://dx.doi.org/10.3389/fonc.2018.00086
Shepshelovich, D., Tibau, A., Goldvaser, H., Molto, C., Ocana, A., Seruga, B., & Amir, E. (2018). Postmarketing modifications of drug labels for cancer drugs approved by the US Food and Drug Administration between 2006 and 2016 with and without supporting randomized controlled trials. Journal of Clinical Oncology, 36(18), 1798-1804. https://dx.doi.org/10.1200/JCO.2017.77.5593
Shimonosono, M., Arigami, T., Yanagita, S., Matsushita, D., Uchikado, Y., Kijima, Y.,…Natsugoe, S. (2018). The association of human endogenous retrovirus-H long terminal repeat-associating protein 2 (HHLA2) expression with gastric cancer prognosis. https://dx.doi.org/10.18632/oncotarget.25179
Varricchi, G., Galdiero, M. R., & Tocchetti, C. G. (2017). Cardiac toxicity of immune checkpoint inhibitors: Cardio-oncology meets immunology. Circulation, 136(21), 1989-1992. https://dx.doi.org/10.1161/CIRCULATIONAHA.117.029626
Wolchok, J. D., Chiarion-Sileni, V., Gonzalez, R., Rutkowski, P., Grob, J.-J., Cowey, L.,…Larkin, J. (2017). Overall survival with combined nivolumab and ipilimumab in advanced melanoma. New England Journal of Medicine, 377(14), 1345-1356. http://dx.doi.org/10.1056/NEJMoa1709684
Xia, Q., Wei, L., Zhang, Y., Sheng, J., Wu, W., & Zhang, Y. (2018). Immune checkpoint inhibitors TIM-3 and PD-1 regulate monocyte and T lymphocyte function in septic patients. (2018). Mediators of Inflammation, 2018, article ID 1632902. https://dx.doi.org/10.1155/2018/1632902
Xu, C., Chen, Y. P., Du, X. J., Liu, J. Q., Huang, C. L, Chen, L.,…Ma, J. (2018). Comparative safety of immune checkpoint inhibitors in cancer: Systematic review and network meta-analysis. British Medical Journal, 363, k4226. https://dx.doi.org/10.1136/bmj.k4226